Contents
What Is Dyspneic?
Dyspneic is often referred to as shortness of breath. Characterized by a feeling of not being able to breathe deeply or quickly enough, it is usually very intense. Obesity, altitude, extreme temperatures, and hard exercise can cause breathlessness in healthier people. However, if shortness of breath is inexplicable, or comes on suddenly for no reason, it could be dyspneic. Dyspneic is not a disease itself, but a symptom of other diseases related to the heart and lungs.
Symptoms of Dyspneic
Notable symptoms include labored breathing which persists for more than a few minutes after exercise or does not completely go away. Breathing can feel too shallow, and in worse cases, the sufferer might feel like they are suffocating. Chest tightness is also another symptom. Dyspneic is more likely if breathlessness comes on suddenly, especially after activities the patient used to find easy but can no longer perform without feeling short of breath.
A doctor should be consulted when there is shortness of breath and:
- It has been persistent for over a month
- It's worse after exercise
- It's worse when lying down
- A persistent cough over 3 weeks
- Swollen ankles
Causes of Dyspneic
Dyspneic is a symptom that may arise from many different conditions. Therefore, its cause can be traced to four areas of illness: cardiac, respiratory, psychogenic, or neuromuscular disease. It can also arise from a combination of illnesses in these areas.
Cardiovascular causes | Respiratory Causes | Psychogenic | Neuromuscular Causes | Other Causes |
Cardiac Arrhythmia Pulmonary Hypertension Pulmonary Edema Congestive Heart Failure Acute Coronary Syndrome Valvular Heart Defect Pericardial Tamponade Intracardiac Shunting | Asthma Congestive Obstructive Pulmonary Disorder (COPD) Pulmonary Embolism Pneumonia Lung Malignancy Aspiration Pneumothorax | Psychogenic Dyspneic Hyperventilation Syndrome Vocal Cord Dysfunction Syndrome Foreign Body Aspiration | Obesity Myopathy Neuropathy Phrenic Nerve Paralysis Kyphoscoliosis Central Nervous System Dysfunction Spinal Cord Dysfunction Chest Trauma | Anemia Liver Cirrhosis Sepsis Anaphylaxis Angioedema Epiglottitis Thyrotoxicosis Metabolic Acidosis Acute Renal Failure |
As well as physiological factors, dyspneic can also be caused by psychological factors, notably anxiety. During a dyspneic episode caused by anxiety suffers may experience any of these symptoms:
- Tightness in chest
- Hyperventilation
- Breathlessness
- Tension in muscles
- Heart palpitations
- Vertigo
- Irritability
- Feeling on edge
- Nausea
Pathophysiology
Dyspneic occurs as a result of the interplay between the signals and receptors in the central nervous system, specifically peripheral chemoreceptors, and mechanoreceptors in the upper airways and lungs.
The area of the brain responsible for respiration is made up of three neuron groupings that work together to coordinate the pace of respiration. Inhalation is directed by the dorsal medulla, whereas exhalation is coordinated by the ventral medulla. The pontine groupings take charge of regulating the frequency and intensity of the signals in the medulla where the pneumotaxic groupings restrict inhalation and the apneustic areas extend and promote inhalation.
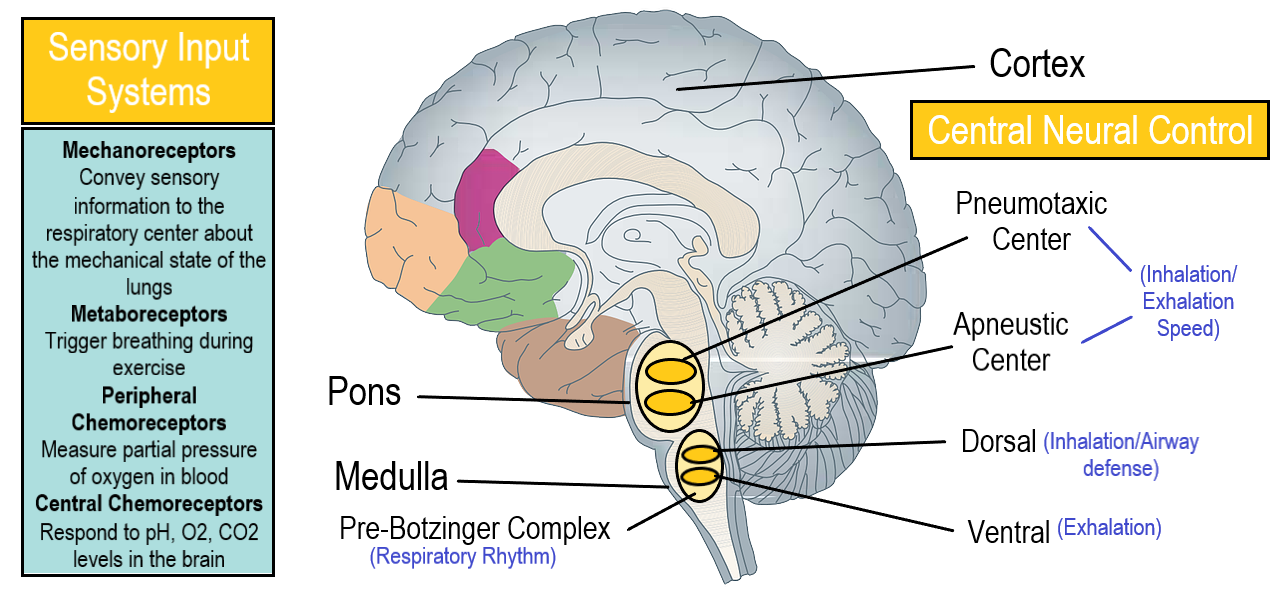
Mechanoreceptors are found in the airways and lungs, and they convey sensory information to the brains' respiratory area. Mechanoreceptors are responsible for monitoring the volume of lung space and looking out for harmful irritants. The receptors signal through the vagus nerve to increase breath rate, volume of oxygen intake, or to encourage coughing in response to air irritants.
Peripheral chemoreceptors, including the carotid and aortic bodies, regulate the partial pressure of arterial oxygen in the blood. The carotid bodies are believed to account for as much as 15% of the power behind respiration. The bulk of power, however, comes from the central chemoreceptors. These receptors are sensitive to pH changes in the central nervous system, and they reside in the ventral medulla. The acidity of these areas dictates ventilation levels, for example when pH goes up to become more alkaline, hypoventilation will happen.
Diagnosis
Only a doctor can accurately diagnose dypsnea. As it is linked to so many diseases there are several tests a doctor may perform.
- A spirometry, or lung function test, may be used to test for asthma and COPD. Spirometry measures lung capacity and respiration speed.
- Blood testing can highlight issues such as anemia, blood clots, infections, and fluid in the lungs.
- An Electrocardiogram (EKG) test may be employed to rule out heart attacks and arrhythmia.
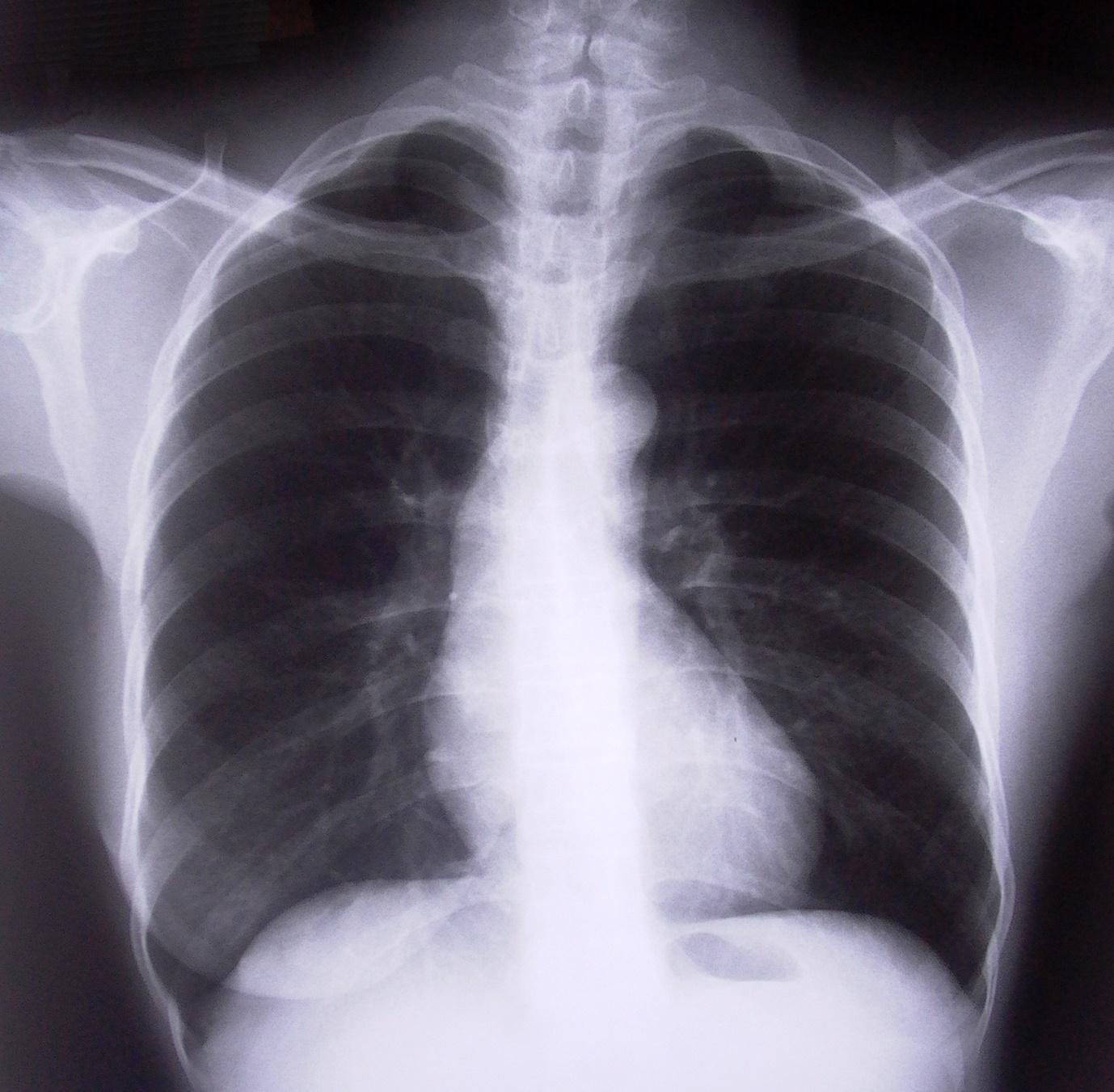
- A chest x-ray or CT scan may be taken to diagnose lung disease, clots, or pneumonia.
- A pulse oximetry text might be performed to measure blood oxygen levels and circulation levels.
Can it Be Cured?
Treatment of dyspneic will depend on what is causing it and will vary from case to case. For example, treatment of dyspneic caused by asthma will be different than if it is caused by obesity.
The MRC breathlessness scale can be used to determine the severity of dyspneic.
Grade | Degree of breathlessness related to activity |
1 | Not troubled by breathless except on strenuous exercise |
2 | Short of breath when hurrying on a level or when walking up a slight hill |
3 | Walks slower than most people on the level, stops after a mile or so, or stops after 15 min walking at own pace |
4 | Stops for breath after walking 100 yards, or after a few minutes on level ground |
5 | Too breathless to leave the house, or breathless when dressing/undressing |
Source: Williams, 2017.
This video details some common treatments:
If obesity is the cause then a doctor will recommend an exercise and weight loss plan to aid in reducing symptoms.
Certain lung conditions including COPD will require seeing a specialist pulmonologist, or lung doctor. More severe conditions may require supplemental oxygen. Pulmonary rehabilitation involves following a program of specific exercise and breathing techniques to help limit the symptoms of dyspneic.

If heart failure is the issue, then cardiac rehabilitation will be necessary to reduce the symptoms of dyspneic. In worse cases, an artificial pump to help the heart may be necessary.
Other treatments include: inhalers, tablets, capsules, liquids, and programs to stop smoking.
Psychological treatments include diaphragmatic breathing exercises that a doctor can teach or a referral to a psychotherapist who can help to alleviate symptoms associated with anxiety.
The NHS gives tips for managing breathlessness yourself in this video:
Here is a short recap from Dr Matt Barton PhD:
See this resource for supporting someone living with dyspneic:
https://supporting-breathlessness.org.uk/
Bibliography
Banzett, R.B., Baker, K., O'Donnell, C., Parshall, M., Lansing, R., Schwartzstein, R. & Stevens, J. (2017) 'A17 MEASUREMENT OF SYMPTOMS AND FUNCTION: Visualizing Mdp Results: The 'dyspneic Profile Graph' Applied To Data From Hospitalized Patients'. American Journal of Respiratory and Critical Care Medicine. Vol. 195. pp. 1.
Elbehairy, A.F., Ciavaglia, C.E., Webb, K.A., Guenette, J.A., Jensen, D., Mourad, S.M., Neder, J.A. & O'Donnell, D.,E. (2015) 'Pulmonary Gas Exchange Abnormalities in Mild Chronic Obstructive Pulmonary Disease: Implications for Dyspneic and Exercise Intolerance'. American Journal of Respiratory and Critical Care Medicine. Vol. 191(12). pp. 1384-1394.
Hashmi, M. F., Modi, P. and Sharma, S. (2023) Dyspneic. In: StatPearls. Florida, US: StatPearls Publishing
Herigstad, M., Hayen, A., Wiech, K. and Pattinson, K. T. S. (2011) 'Dyspnoea and the brain'. Respiratory Medicine. Vol. 105(6). pp. 809-817
Kolman, K. B. and Losey, K. R. (2018) 'Worsening dyspneic', Journal of Family Practice. Vol.67(1). pp. 39–42.
Williams, N (2017) 'The MRC breathlessness scale'. Occupational Medicine. Oxford: England. Vol.67 (6). pp.496–97.